
You started HRT and felt better, for a while. Or maybe you never felt better at all. Either way, you're still symptomatic, and the standard advice is to wait longer or adjust the dose. Here's what's actually happening in the four most common HRT under-response patterns, why single-point testing misses them, and what the hormone data looks like when treatment genuinely isn't working.

You started HRT and felt better, for a while. Or maybe you never felt better at all. Either way, you're still symptomatic, and the standard advice is to wait longer or adjust the dose. Here's what's actually happening in the four most common HRT under-response patterns, why single-point testing misses them, and what the hormone data looks like when treatment genuinely isn't working.
You started hormone therapy (HT) because you wanted relief.
Instead, you're still exhausted, still anxious, still waking at 3am. And now you're wondering whether HT simply doesn't work for you.
It might not be that. In fact, it probably isn't.
Maybe the hot flashes eased at first. Sleep improved briefly. And then, a few months in, something shifted, symptoms came back, or never fully left. The brain fog is still there. The mood crashes still arrive without warning.
You go back to your provider. Your labs look fine. You're told to give it more time, or to try a different dose, or that HT isn't for everyone.
What is less often discussed is that HT under-response is not random, and it is not rare. It follows recognizable patterns, patterns that are visible in hormone data and that standard single-point testing is structurally unlikely to catch.
Understanding which pattern applies to you changes what your next step should be. And it changes the conversation you can have with your provider.
Why "My Labs Look Fine" Doesn't Always Tell the Whole Story
Standard HT monitoring typically involves a blood draw, often at a single point in time, often not timed to any particular phase of the cycle or time of day relative to application. If the result falls within the laboratory reference range, treatment is typically considered to be on track.
The problem is that hormone levels on HT are not static. Estradiol from a patch, gel, or cream fluctuates across the day and across the week. Absorption varies based on application site, skin hydration, body composition, and individual metabolic differences. A measurement taken at the right moment on one day might look completely different from a measurement taken 12 hours later or on a different day of the week.
A single number tells you what your hormone level was at one moment. It tells you nothing about whether that level is stable enough to provide consistent symptom relief, whether it's adequate specifically during the symptomatic windows you're experiencing, or whether the pattern across a week or a cycle is one that matches what your body needs.
This is the gap behind HT under-response: levels that look adequate on paper may not be sufficiently addressing your symptoms.
As we explore in our guide to knowing if your HRT dose is right, the question isn't just what your level is, it's whether it's doing what it needs to do, when you need it to do it.
The Four HRT Under-Response Patterns
Not all HT under-response looks the same. Most cases fall into one of four distinct patterns, each with a different mechanism and a different clinical path forward.
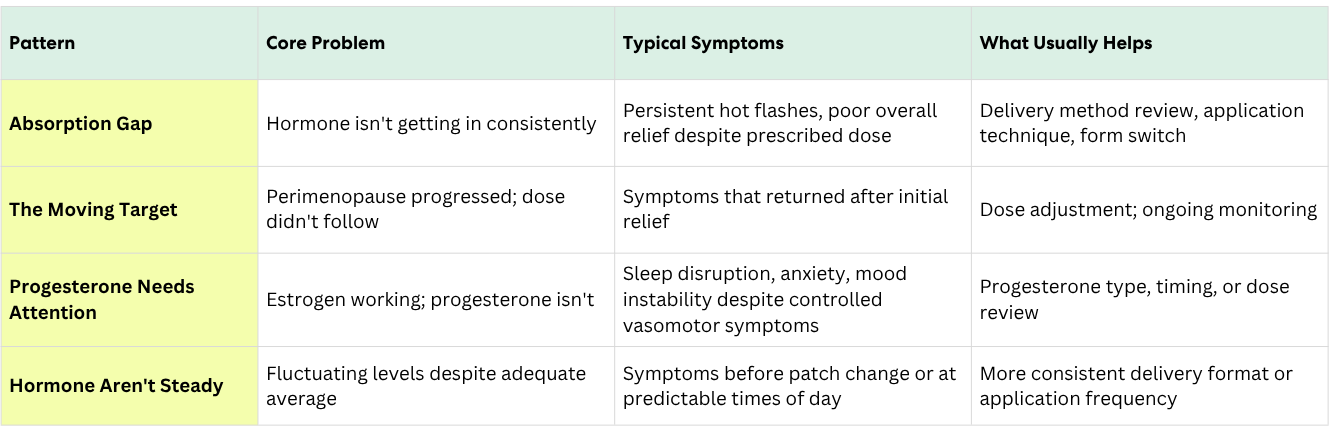
Pattern 1: The Absorption Gap
One of the more common under-response patterns, and one that is often overlooked. The prescribed dose is theoretically adequate, but absorption is inconsistent, meaning the hormone isn't reliably reaching systemic circulation at the level needed.
Absorption issues are more common than most women are told. Transdermal estradiol (patches, gels, creams) bypasses the liver but depends on skin absorption, which varies significantly between individuals. Factors that affect absorption include skin thickness and hydration, application site rotation (or lack thereof), body composition, and even heat and exercise. A woman who applies her estrogen gel in the morning and showers within the hour may be absorbing a fraction of what was prescribed.
The signal in the data: hormone levels that look lower than expected for the prescribed dose, or that vary significantly between measurements. As we discuss in the guide to estradiol forms, the delivery method itself may need to change, not just the dose.
What helps: considering application technique, delivery form, or timing of medication may be useful. For women on oral estradiol, the conversation may include whether transdermal delivery would be a better fit.
Pattern 2: The Moving Target
The dose was right at initiation. But perimenopause didn't stop progressing just because the prescription was written.
This is the pattern women describe most often in clinical consultations: I felt so much better for the first few months. And then something shifted. The prescription stayed the same. The transition didn't.
Perimenopause is not a static condition. The four hormone patterns of perimenopause shift over time as ovarian function continues to change. A dose that adequately replaced estrogen six months ago may no longer be sufficient as endogenous production declines further. The hormonal target moved. The dose didn't follow it.
This pattern produces a very recognizable trajectory: genuine initial relief, followed by a slow erosion of efficacy over weeks or months, not a sudden failure, but a gradual return of the symptoms that HT had quieted.
What this often looks like: hormone readings that have stayed relatively consistent, alongside a gradual return of symptoms that HT had quieted in the first several months. This is distinct from Pattern 1 because absorption isn't the problem. Adequacy for current hormonal needs is.
What helps: a dose adjustment, sometimes combined with monitoring to confirm the new level actually holds. But because the transition continues, this is not a one-time fix, since the transition itself continues to move. This is exactly why your HT can stop working even when nothing in the prescription changed.
Pattern 3: When Progesterone May Need Attention
For some women whose symptoms persist on HT, the estrogen side of the prescription is working as expected, and the progesterone side is another angle that could be modified.
For most women, progesterone is well tolerated and does important work, both in protecting the uterine lining and in supporting mood, sleep, and a sense of calm. Micronized progesterone (Prometrium) has a downstream effect that acts on the brain's GABA receptors. GABA is the brain's main calming pathway, and when it is activated, the effect is generally calming and sleep-supportive. For a smaller group of women, the same pathway can produce the opposite effect, low mood, anxiety, or sleep disruption that does not ease over time.
The progesterone picture can also be complicated by the type of progestogen a woman is taking. Synthetic progestins, such as medroxyprogesterone, have somewhat different effects than micronized progesterone. Some women feel better on synthetic forms, others on micronized. There is no universal ranking, and the most reliable way to know which suits a particular woman is to observe symptom changes over time on each.
What this often looks like in practice: an HT regimen that has eased hot flashes and other estrogen-responsive symptoms, but where insomnia, anxiety, or mood instability has not improved, or has come back. Recognizing that pattern is what matters, since the next step may involve a conversation with your provider about the type, timing, or dose of progesterone, and adjustments here can sometimes produce a noticeable change within days rather than weeks.
The takeaway is not that progesterone is the part of HT to worry about. For most women, it is well tolerated and doing important protective work. For the smaller group who do not feel well on a particular form, knowing that variability exists, and that alternatives are worth discussing with a provider, is what allows the issue to be addressed rather than endured.
Pattern 4: When Hormone Levels Aren't Steady Throughout the Week
For some women, an HT prescription works well overall, but symptoms may come back at some predictable times. This often happens because hormone levels can vary across the days of the week or across a single day, and symptoms often return when levels are fluctuating.
This pattern is more common with certain delivery formats. A twice-weekly patch can produce a lower window in the day or two before the next patch is applied. Once-daily gels and creams can rise and fall across each 24-hour period. A woman on either format may feel well much of the time and then notice that her symptoms reliably worsen at certain hours or on certain days.
The most recognizable signal here is the timing of the symptoms themselves: hot flashes that consistently return in the evening when using a morning gel, sleep disruption or mood changes in the day or two before a patch change, a pattern that repeats from week to week. For Oova users on hormone therapy, the rise and fall of urinary estrogen metabolite may follow a similar rhythm. While a urine measurement is not a direct equivalent of a serum estradiol value, it can reflect how a dose is being absorbed and processed across the days. When that rhythm lines up with the timing of a woman's symptoms, it points toward a hormonal cause worth exploring with her provider. When it does not line up, that is also useful information, since it can suggest looking elsewhere for what may be driving the symptoms.
If you recognize a pattern like this in your own experience, with or without hormone data alongside it, it is worth bringing to a conversation with your provider. There are several approaches a provider may consider together with you, including a change in patch schedule or delivery format. Decisions about dose or regimen are best made with your provider's guidance.
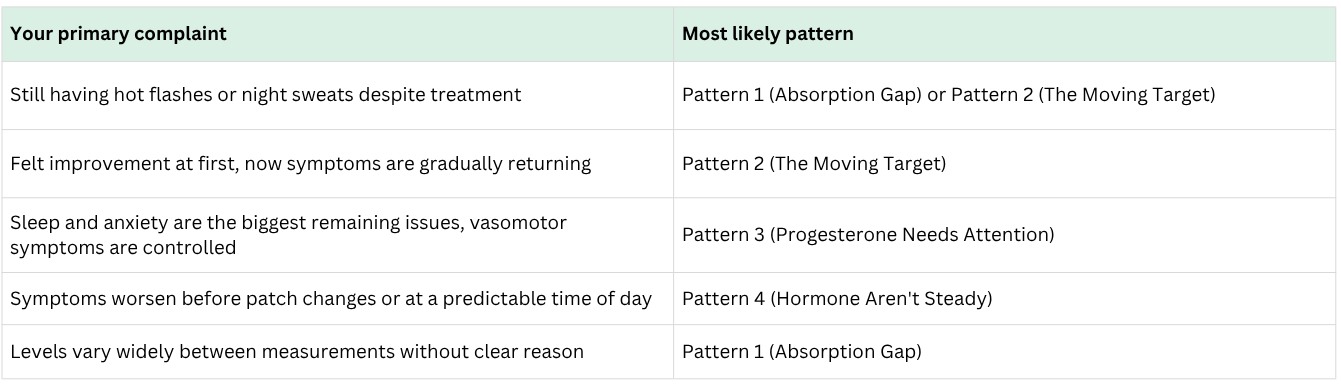
Which Pattern Sounds Most Like You?
Before moving to the next section, it's worth pausing to identify where you are. Most women fit primarily into one pattern, though two can coexist.
The Four HRT Under-Response Patterns at a Glance
Two Women, Same Prescription, Different Stories
Consider two women, both on the same estradiol patch dose and oral micronized progesterone, both still symptomatic six months into treatment.
The first woman has hormone readings that swing widely from one day to the next. Some days her levels look adequate, other days noticeably lower. This pattern could be reflective of one or both of the following situations: variability in how the hormone is being absorbed, where the prescribed dose may not be consistently reaching adequate levels in her body, or ongoing ovarian fluctuation, where her own hormone production is still rising and falling underneath the steady prescription. Her symptoms tend to be more pronounced on the days when her overall levels run lower.
The second woman has steady hormone readings from week to week. Her levels are not varying significantly, but her symptoms have been gradually returning over the past several months. This pattern is more consistent with the moving target, her perimenopause has progressed further since she started HT, and the dose that worked at initiation may no longer match where her body is now.
Both women are doing everything right. Both are still symptomatic. But the path forward looks different for each. For the first woman, the next step may involve a conversation about how the dose is being delivered and absorbed, or about whether her ovarian fluctuation is contributing to the variability she is seeing. For the second woman, the next step may be a conversation about whether the dose itself is sufficiently covering her symptoms.
The pattern over time tells a different story for each woman, and a clearer story than any single moment can, and a clearer story than any single lab value would reveal.
What Daily Tracking Can Add
The first 90 days of HT are when many women and their providers are looking to see whether treatment is helping. A single test gives you one moment in time. It cannot easily show whether your hormone levels are steady from day to day, whether they shift in the days before a patch change, or whether the times you have felt better line up with particular hormonal patterns.
Daily hormone tracking adds context that a single test does not. A woman tracking her hormones over a week or two can see whether her levels are steady or variable, and whether the days she felt symptomatic line up with shifts in her own data. Over time, she can see whether a change in her hormone regimen improves her symptoms, and whether that lines up with what her hormone levels are doing.
Finding the right HT approach often takes more than one conversation. Having a picture of how things have moved between visits, rather than relying on memory or a single result, gives both the woman and her provider more to look at together when deciding on next steps.
What to Track and What to Bring to Your Provider
If you're on HT and still symptomatic, these are the questions worth answering before your next appointment, ideally with data rather than memory:
Are your symptoms following a predictable schedule within the week or the day? If hot flashes, insomnia, or mood shifts reliably worsen at a certain point, before a patch change, in the evening, the week before your next dose, that temporal pattern is clinically meaningful. It points toward Pattern 4.
Have your symptoms been gradually returning after an initial improvement? That trajectory suggests Pattern 2, the dose may need revisiting based on where the transition has progressed to, not where it was when you started.
Are your sleep and anxiety symptoms dominant, even though vasomotor symptoms are controlled? That symptom profile, good estrogen response, persistent neurological symptoms, is the signature of Pattern 3. Worth asking your provider specifically about progesterone type, dose, and timing. See also low vs. high progesterone symptoms for more context.
Are your measured levels inconsistent or lower than expected for your dose? That's Pattern 1. Application site, technique, skin condition, and delivery form are all worth reviewing.
Specific observations like this give a provider more useful information to work with than "I still feel terrible." The goal is not to arrive at your appointment with a diagnosis, but rather to have a productive discussion.
The Difference Between Waiting and Watching
Some symptoms on HT take time to respond, such as vaginal dryness and changes in bone density. Waiting with regard to these symptoms is reasonable.
When symptoms that should be improving are not, waiting alone is different from watching or monitoring. Watching means paying attention to the pattern, both in how you feel and in what your hormone data shows. It means seeing whether the days your symptoms returned line up with shifts in your hormone data, or whether the two seem unrelated. It means having something to bring to your next appointment beyond memory of how the past few weeks felt.
This is not about replacing your provider's judgment with your own. It is about giving both of you something more to look at together, so that the next conversation can build on what the previous one started.
Note: this article focuses on under-response, why HT isn't relieving symptoms adequately. If your question is different, why your response differs so markedly from another woman on the same protocol, that's a separate but related topic about individual variability in estrogen and progesterone sensitivity, metabolism, and treatment expectations, which we cover in Why Some Women Thrive on HRT and Others Feel Worse.
If your HT isn't working the way you expected, don't settle for "your labs look fine." See the hormone pattern behind your symptoms, and bring something more useful than guesswork to your next appointment. Start tracking your hormone pattern →
About the author
Sources
- Stuenkel CA, et al. "Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline." Journal of Clinical Endocrinology & Metabolism. 2015;100(11):3975–4011.
- Stanczyk FZ, et al. "Pharmacokinetics and potency of progestins used for hormone replacement therapy and contraception." Reviews in Endocrine and Metabolic Disorders. 2002;3(3):211–224.
- Kuhl H. "Pharmacology of estrogens and progestogens: influence of different routes of administration." Climacteric. 2005;8(Suppl 1):3–63.
- Röst A, et al. "Variability of transdermal estrogen delivery and its clinical implications." Maturitas. 2019;124:1–6.
- Prior JC. "Progesterone for Symptomatic Perimenopause Treatment." Facts Views Vis Obgyn. 2011;3(2):109–120.
- Pinkerton JV, et al. "The Menopause Society 2023 hormone therapy position statement." Menopause. 2023;30(4):321–326.
- Glaser R, Dimitrakakis C. "Testosterone therapy in women: myths and misconceptions." Maturitas. 2013;74(3):230–234.
About the Oova Blog:
Our content is developed with a commitment to high editorial standards and reliability. We prioritize referencing reputable sources and sharing where our insights come from. The Oova Blog is intended for informational purposes only and is never a substitute for professional medical advice. Always consult a healthcare provider before making any health decisions.



